Varicose Veins
Varicose vein disorders are very common and affect especially the lower limb. In total 20 percent
of the population suffer from varicose veins and 2 percent have skin changes that may produce venous ulceration.
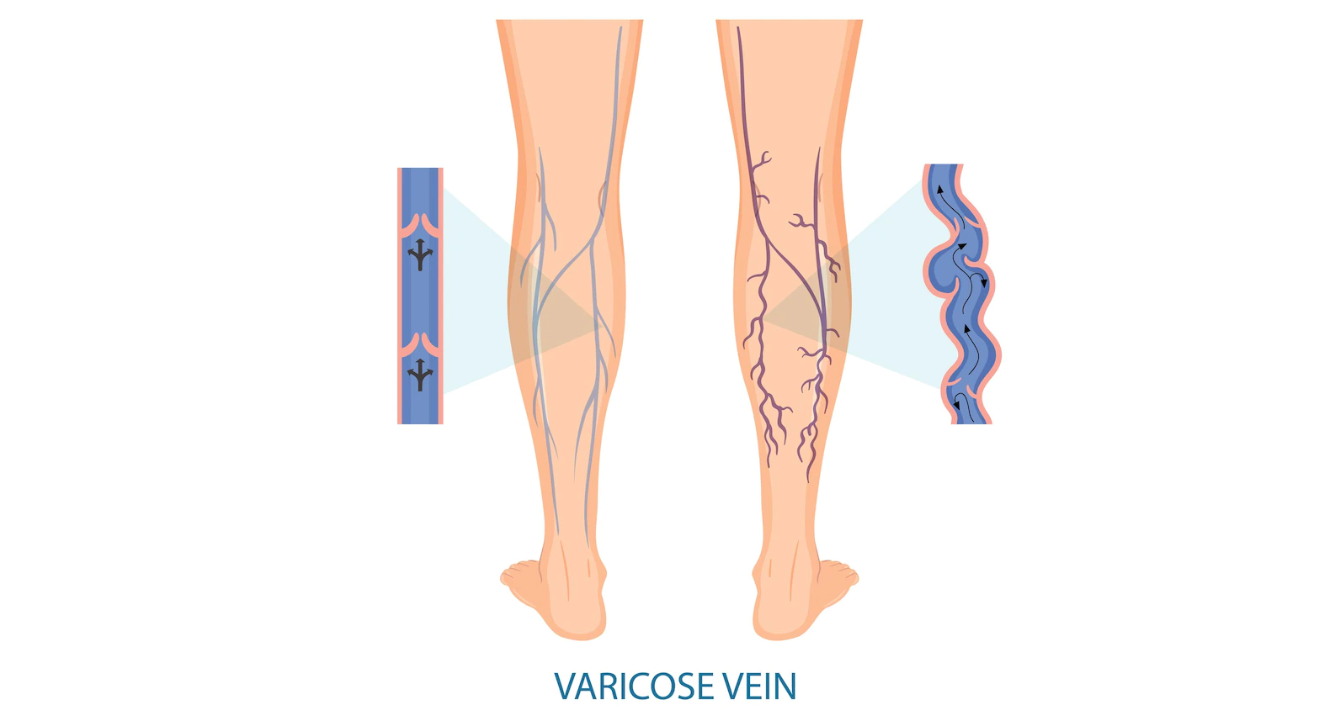
DEFINITION OF VARICOSE VEIN:
When a vein becomes dilated, elongated, and tortuous, the vein is said to be a varicose vein.
SITES :-
The common sites of varicosity are:
The superficial venous system of the lower limbs affects either the long saphenous or the short saphenous vein or both.
Esophageal varix [affecting veins of the gastro-esophageal junction]
Varicosity of hemorrhoidal vein [piles]
Varicosity of the spermatic veins [varicocele]
AETIOLOGY:
Morphological factor:
Varicose veins of the lower limbs are the penalty for human beings to pay for their erect posture.
The veins have to drain against gravity. The superficial veins have loose fatty tissue to support them and thus suffer from varicosity. there are three types of varicosities.
Primary varicose vein.
Secondary varicose vein.
Congenital varicose vein.
Primary varicose vein
This condition is commonly seen, mainly due to defects in the valves. the defects may be congenital or acquired.
Defect in the saphenofemoral valve leads to varicosity of the long saphenous vein.
Defect in the saphenopopliteal valve leads to varicosity of the short saphenous vein.
Defects in the valves of the perforators lead to varicosity of either long or short saphenous system.
The mechanism that causes the superficial vein valves to fail has not been fully established.
what appears to happen is that first, a small gap appears between the valve cups at the commissure (where the valve leaflets join the wall).
Which gradually widens resulting in more reverse blood flow (venous reflex) allowed.
The valve cups get degenerated and holes develop in them eventually they disappear completely,
and the vein below the valve responds by getting dilated. varicose veins may eventually reach five times the usual size if left to develop for a long time.
Secondary varicose vein
Mechanical factors- e.g. during pregnancy under the influence of estrogen and progesterone which
causes the smooth muscle in the wall to relax, tumors in the pelvis, (cancers of the ovary, rectum, uterus, etc.)
Deep vein thrombosis leads to damage to the valves.
Hormonal cause
Acquired arteriovenous fistula
Retroperitoneal lymphadenopathy.
Iliac vein thrombosis.
Congenital Varicose Vein
Occasionally varicose veins may develop below 20 yrs. Age. These are mostly due to congenital arteriovenous fistula.
Predisposing Factors -
Prolong Standing :- because of prolonged standing,
a long column of blood along with gravity plus pressure on the weakened valve of the vein causes failure of the valve and results in varicose veins.
Obesity :- excessive fatty tissue in the subcutaneous tissue offers poor support to the vein. this leads to the formation of varicosity.
Pregnancy :- Pregnancy (1) Estrogen and progesterone cause dilatation and relaxation of the veins of the lower limb
(2)Pregnant uterus-causes pressure on the inferior vena cava thus causing obstruction to the Venous flow
Old Age :- This causes atrophy and weakness of the vein valve, at the same time with aging the valve in the vein becomes gradually incompetent.
Athletes :- forcible contraction of the calf muscle may force blood through perforating vein in the reverse direction,
which causes destruction of the valve and leads to the formation of a varicose vein.
SYMPTOMS :-
The commonest symptoms are tired and aching sensation in the affected lower limb, particularly in the calf.
Sharp pain
Some patients may suffer from cramp in calf region.
Dilated and tortuous veins of the leg.
Ankle swelling.
Hyperpigmentation- Black color skin
Eczema.
Venous ulcer.
TREATMENT:-
Conservatively disease can be managed with compression stockings and foot elevation.
Surgical management consists of ultrasound-guided foam sclerotherapy,
ELVA (Endo Venous Laser Ablation), RFA (Radio Frequency Ablation), Saphenofemoral ligation and Long saphenous vein stripping, skin grafting, etc.
Compression Stockings
Compression Stocking relies on graduated external pressure to improve deep venous return.
Compression stockings that can be knee length or thigh length and should be regularly used.
The incorrect application of compression hosiery can have serious consequences
(pressure necrosis, tourniquet effects); thus assessment, prescription, and application
of compression hosiery should be limited to those with the appropriate skills and training.
Ultrasound-Guided Foam Sclerotherapy
Ultrasound-guided foam sclerotherapy involves the injection of detergent directly into the
superficial veins. The detergent destroys the lipid membranes of endothelial cells causing
them to shed, leading to thrombosis, fibrosis, and obliteration (sclerosis). The procedure commences with the patient standing,
and the sites of venous cannulation are selected and marked using ultrasound.
Then, with the patient supine, the major venous trunks and superficial varicosities to be treated are all cannulated using ultrasound guidance.
Endo Venous Laser Ablation
Endo venous laser ablation (EVLA) as a treatment for varicose veins was first described in 2001, and involves the insertion of a laser fiber into
the lumen of an incompetent truncal vein, with subsequent thermal ablation of the vein. The vast majority of patients with primary and recurrent
varicose veins are suitable for EVLA, with success reported in treating the long, short, and anterior saphenous veins, perforators, and varicosities themselves.
The factors which may preclude EVLA pertain to either the patient (unsuitable for local anesthesia, e.g. needle phobia) or the vein (excess tortuosity, thrombophlebitis).
Radiofrequency Ablation.
Radiofrequency ablation (RFA) is a minimally invasive endovascular
therapy that uses a bipolar catheter to generate thermal energy to ablate the vein.
Preoperative planning and consent, patient positioning,
tumescent anesthesia administration, and postoperative management are identical to EVLA.
The main differences include vein cannulation and method of ablation.
Other Surgical treatment Includes-
Saphenofemoral ligation and long saphenous stripping
Sapheno-popliteal junction ligation and lesser saphenous stripping
Perforator ligation